EEG Sample: The Learning EEG (learningeeg.com)
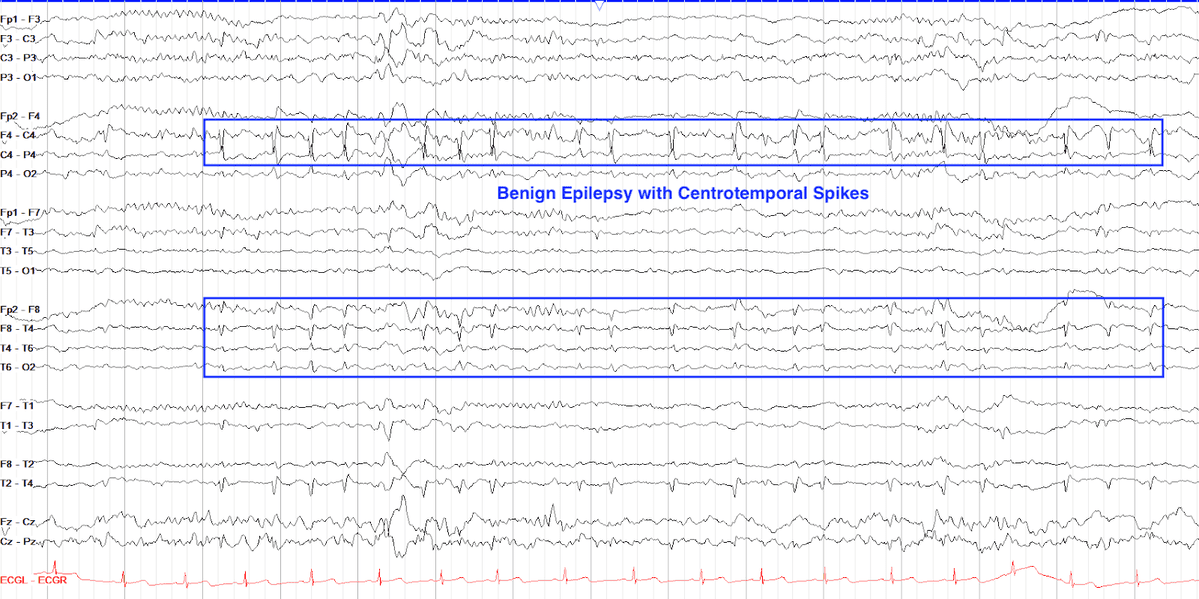
Rolandic spikes are high amplitude waveforms that occur in the centrotemporal regions they appear asymmetrically (unilateral) or bilaterally shifting. Most of the time are asynchronous as well. Rolandic spikes are a paroxysmal activity appearing during wakefulness and are often activated with drowsiness and sleep. The morphology is a spike followed by a slow wave that can occur in trains. The duration of the waveform technically falls in the sharp category (70-200ms) instead of a true spike (<70ms). Rolandic spikes have a triphasic negative peak followed by small positive peaks. This pattern is a normal variant and is benign.
However not all spike discharges from centrotemporal regions are benign.
Question:
Which self-limiting epilepsy is distinctly associated with this paroxysmal activity?
Results
#1. Which self-limiting epilepsy is distinctly associated with this paroxysmal activity?
Childhood epilepsy with centrotemporal spikes previously known as Benign childhood epilepsy with centrotemporal spikes (BCECTS), benign epilepsy with centrotemporal spikes (BECTS) or benign Rolandic epilepsy (BRE) is the most common epilepsy syndrome in childhood, it accounts approximately 20% of all childhood epilepsies. Typical onset is between 3 and 14 years of age, peak is 8 and 9 years of age. BCECTS is inherited, it is self-limiting, and children grow out of this epilepsy in their teen years.
Clinically, children affected will have nocturnal seizures with clonic movements of the mouth and gurgling sometimes with ictal emesis. About 80% of these seizures will occur exclusively in sleep. Unilateral paresthesia of tongue, lips, cheek, and gum and/or unilateral tonic–clonic activity of facial and pharyngeal/laryngeal muscles, on the contralateral side of the focal spike activity will occur. In addition, unilateral facial spasms can progress to the ipsilateral extremities. On the EEG an electro decremental pattern or flattening is followed by rhythmic spike bursts then spike-wave discharges. Unless the seizure secondarily generalizes, which is common, the seizure will end with no postictal slowing.
The interictal background EEG can be normal or with unilateral or bilateral epileptiform discharges maximal over the inferior Rolandic region. Rolandic spikes are maximum at C5 or C6, whereas symptomatic temporal lobe seizures likely have a maximum at T3 or T4.



